Many people with bipolar disorder are first misdiagnosed with post-traumatic stress disorder (PTSD)—and for good reason. The symptoms of PTSD can look remarkably like those of bipolar disorder: intense mood swings, irritability, flashbacks, panic attacks, emotional numbing, and periods of hyper-arousal. The symptoms of PTSD and bipolar disorder can overlap, making it challenging to diagnose and treat both conditions simultaneously. Here are some of the symptoms that may co-occur in individuals with both conditions:
The symptoms of PTSD and bipolar disorder can overlap, making it challenging to diagnose and treat both conditions simultaneously. Here are some of the symptoms that may co-occur in individuals with both conditions:
• Mood instability: Both conditions involve rapid mood changes and emotional dysregulation.
• Sleep disturbances: Insomnia and nightmares are common in both disorders
• Irritability and anger: These emotions can be prominent in both manic episodes and PTSD hyperarousal
• Difficulty concentrating: Cognitive impairments are often reported in both conditions
• Impulsivity: This can be a feature of manic episodes in bipolar disorder and a symptom of PTSD
Understanding these symptoms is crucial for effective management and treatment of both PTSD and bipolar disorder. It is important to seek professional help for accurate diagnosis and tailored treatment plans.
Sharing this checklist and your history with your therapy team may help reveal if panic attacks are a symptom and not the whole diagnosis.
Misdiagnosing bipolar disorder as PTSD (or vice versa) can delay the right treatment. In some cases, trauma-focused therapy can trigger manic symptoms or deepen depression if the underlying mood instability isn’t stabilized first.
Understanding whether you have both—as many do—is key to creating a treatment plan that works.
• Flashbacks and dissociation in PTSD can resemble manic or psychotic symptoms.c or anxiety attacks that appear out of nowhere, without clear triggers.
• Hypervigilance and anxiety mimic early manic warning signs
• Emotional shutdown and numbness can look like depression.
• Mood swings in PTSD (especially in complex trauma or C-PTSD) may appear bipolar.
• Survivors of trauma often develop coping behaviors that resemble hypomania (overachieving, risk-taking, compulsive productivity)
Note. Author-created table based on diagnostic criteria from APA (2022), Judd et al. (2003), and Goodwin & Jamison (2007).
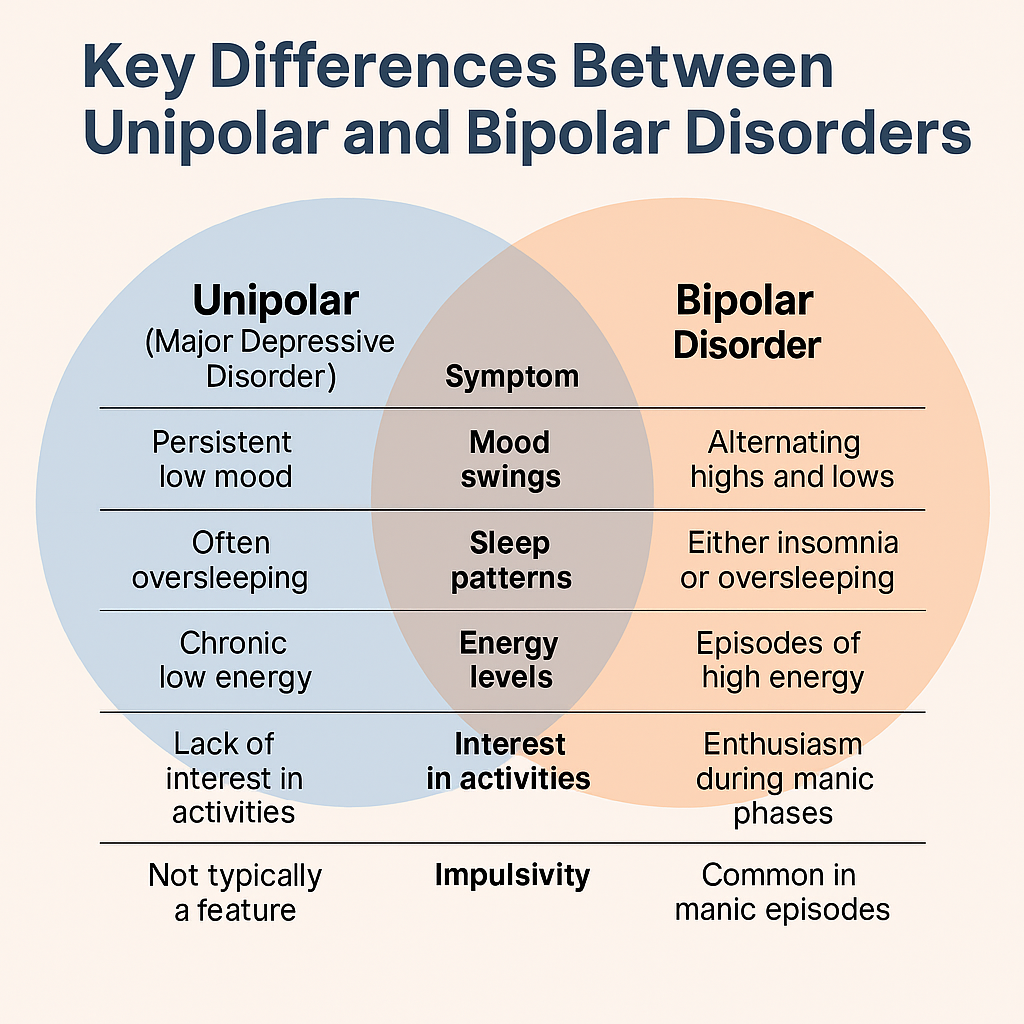
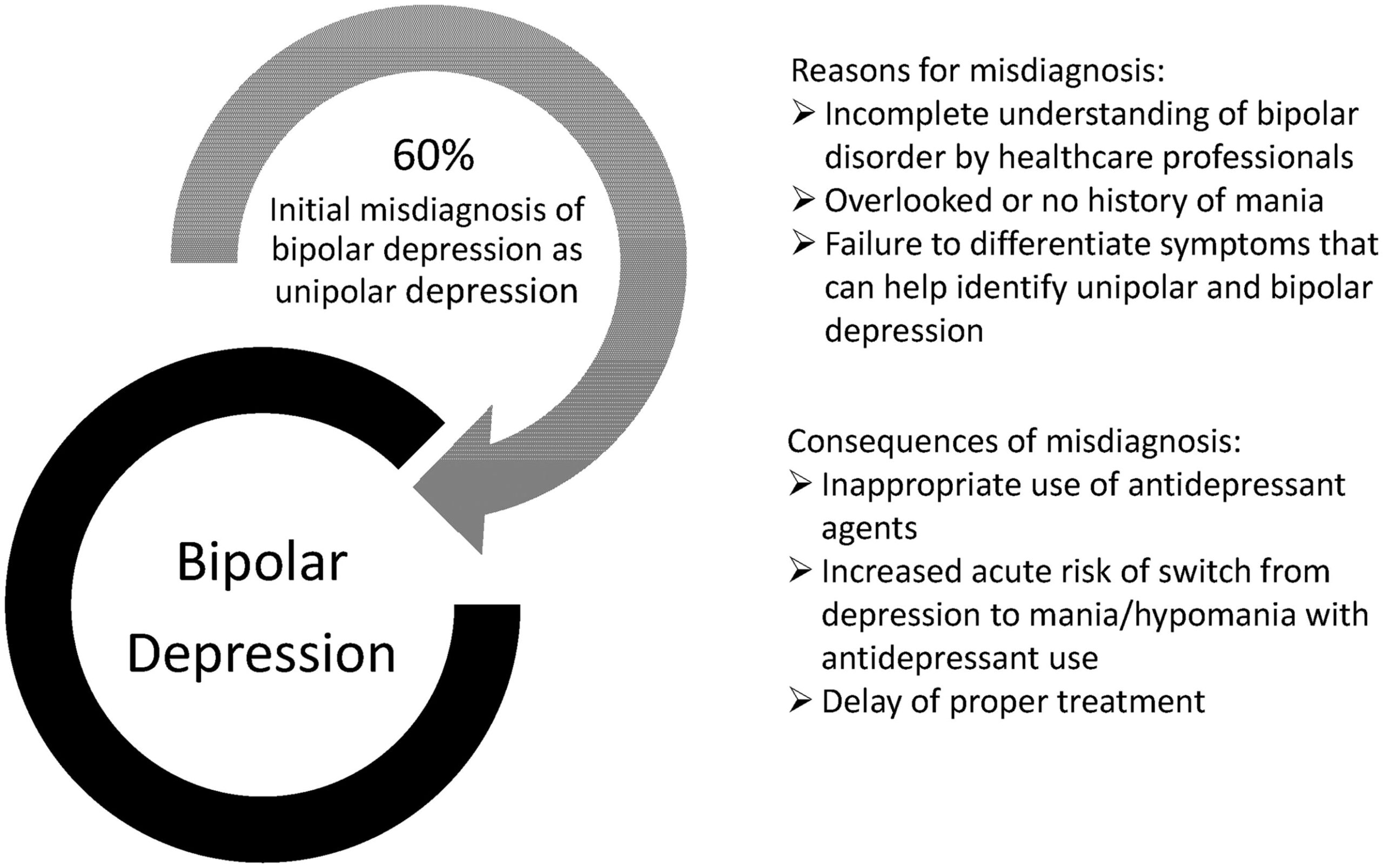
Figure 2. Key Differences Between Unipolar Depression (MDD) and Bipolar Disorder (Types I & II) Note. Author-created infographic based on diagnostic criteria from the American Psychiatric Association (2022), Judd et al. (2003), and Goodwin & Jamison (2007). This image is not sourced from a peer-reviewed publication but visually summarizes established clinical differences. Figure 4. Rates and consequences of misdiagnosing bipolar depression as unipolar depression Note. Adapted from McIntyre, R. S., Soczynska, J. K., Cha, D. S., & Alsuwaidan, M. (2019). Recognizing bipolar depression in clinical practice: How to identify and differentiate it from unipolar depression. Current Medical Research and Opinion, 35(10), 1685–1698.
https://doi.org/10.1080/03007995.2019.1636017. • Repeated relapses
• Worsening depression or anxiety
• Missed medication opportunities (e.g., mood stabilizers)”
• Increased risk of suicide or dangerous behavior
Getting the correct bipolar diagnosis allows for proper treatment, safer medication use, and better long-term outcomes. It also lets families understand patterns that may go back generations.
• Anxiety paired with chronic insomnia, racing thoughts, or impulsive behavior.
• Feeling “charged” or “over-revved” instead of just nervous.
• Anxiety meds helping only temporarily—or make things worse.”
• Frequent cycling between restlessness and exhaustion
Getting the correct bipolar diagnosis allows for proper treatment, safer medication use, and better long-term outcomes. It also lets families understand patterns that may go back generations.
Sections and individual appendices with checklists and other tools are available as both PDFs and interactive HTMLs at
themisfittoyproject.com.
The website offers features the book cannot — such as the ability to create a personalized
These tools help capture important needs, concerns, and patterns — especially when memory is impacted by illness. Bringing a companion or using these tools during appointments can help ensure symptoms and questions are addressed effectively. Tools will be updated regularly based on feedback from readers, professionals, advocates, and families. Suggestions, corrections, or collaborations can be submitted via the
Contact page. These materials are adapted from The Misfit Toy – A Long Winding Story to Get Help and Healing! by Ted Livernois. While the author does not hold clinical credentials, the insights shared come from lived experience with bipolar disorder and neurodivergence.Why PTSD and Bipolar Disorder Are Commonly Confused
📊 Key Differences Between MDD and Bipolar Disorder
Symptom
MDD (Unipolar Depression)
Bipolar Disorder (Type I & II)
Manic episodes
Never present
Present in Bipolar I (full mania); Hypomania in Bipolar II
Depressive episodes
Required for diagnosis; often chronic
Present in both types; usually alternating with elevated or mixed states
Mood cycles
May be long-lasting and episode-based
Clearly cyclical; includes ups (mania/hypomania) and downs (depression)
Energy levels
Consistently low or fatigued
Alternate between high (mania/hypomania) and low (depression)
Sleep patterns
Insomnia or hypersomnia from low mood
Decreased need for sleep during mania; insomnia or hypersomnia during depression
Irritability
Present mostly during depressive lows
Common during mania/hypomania and depression
Self-esteem
Low self-worth, guilt, hopelessness
Inflated self-esteem or grandiosity during manic states
Risky behavior
Rare
Often seen in mania/hypomania (spending, sex, impulsivity)
Psychosis
Possible in severe depression
Possible in manic or depressive episodes (especially Bipolar I)
Diagnosis challenge
Often diagnosed earlier; more straightforward
Often misdiagnosed as MDD before mania/hypomania appears
 Why Getting the Right Diagnosis Matters, treating Panic Attacks alone without addressing an underlying mood disorder can lead to:
Personal Red Flags to Watch For
Why Getting the Right Diagnosis Matters, treating Panic Attacks alone without addressing an underlying mood disorder can lead to:
Personal Red Flags to Watch For
 📚 Resources
📚 Resources
https://www.psychiatry.org/psychiatrists/practice/dsm
https://global.oup.com/academic/product/manic-depressive-illness-9780195135794
https://doi.org/10.1016/S0165-0327(02)00332-0
https://doi.org/10.1001/archgenpsychiatry.2011.12
https://doi.org/10.1111/j.1399-5618.2010.00762.x
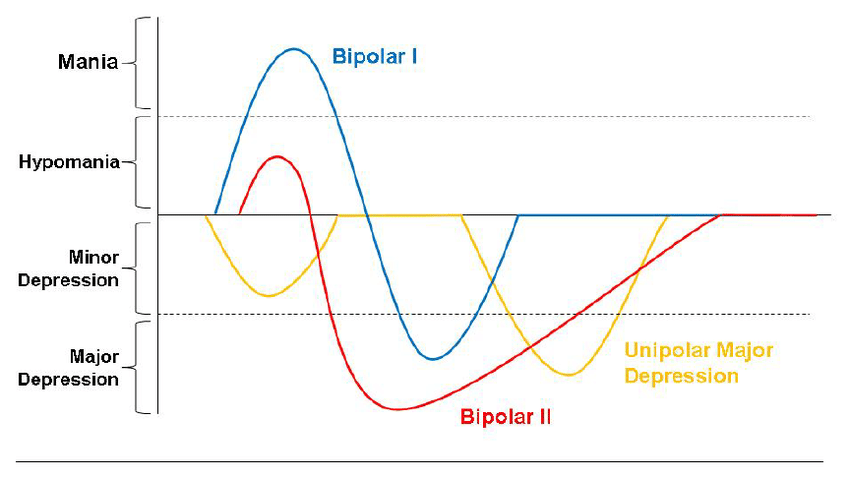
https://www.researchgate.net/figure/Prototypical-Courses-of-Illness-for-Bipolar-Subtypes-in-Contrast-to-Unipolar-Major_fig1_266869236
![]() Care Folder
to share with healthcare professionals, psychiatrists, advocates, loved ones, or hospital teams.
Care Folder
to share with healthcare professionals, psychiatrists, advocates, loved ones, or hospital teams.